
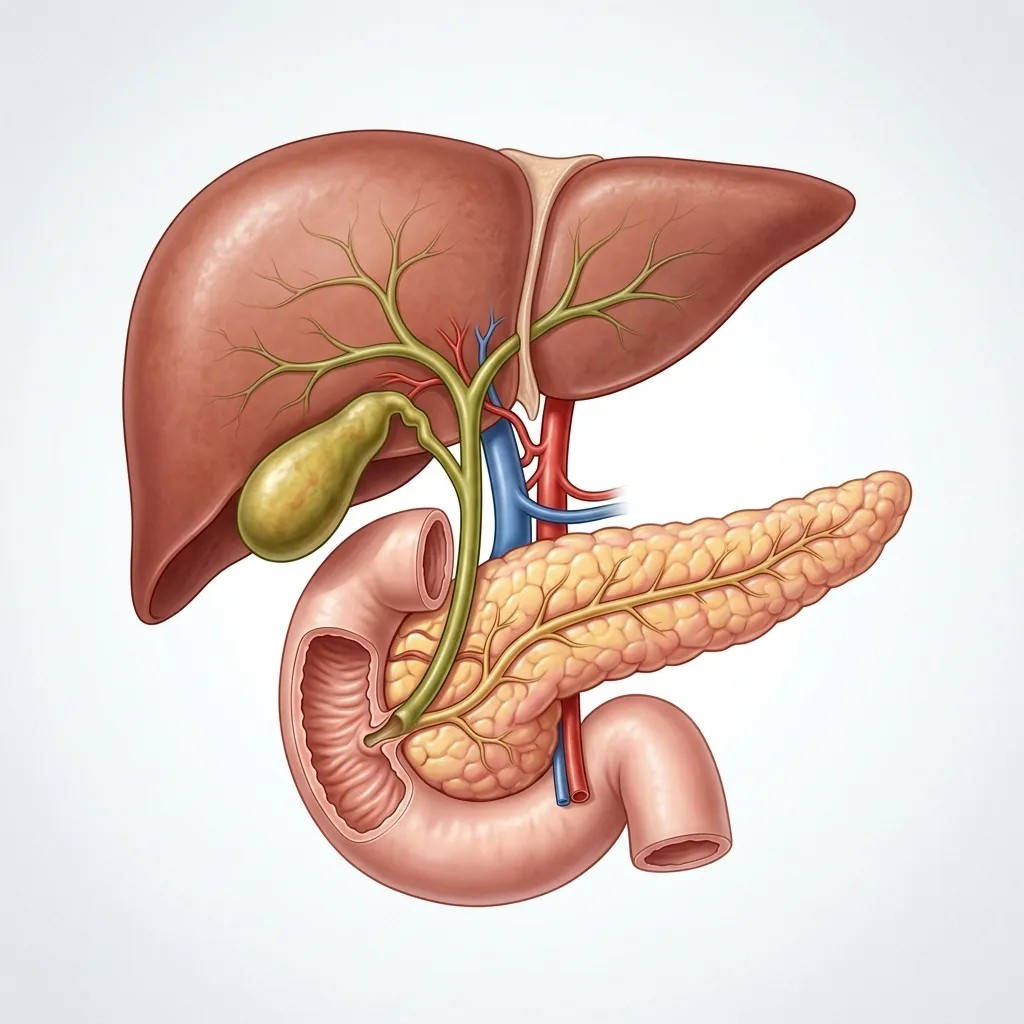
The biliary and pancreatic systems play a critical role in digestion. The liver produces bile, which is stored in the gallbladder and transported to the small intestine via the bile ducts. Simultaneously, the pancreas produces essential digestive enzymes. When blockages occur in these intricate channels—due to stones, strictures, or tumors—it can trigger severe abdominal pain, yellowing of the skin (jaundice), life-threatening infections, or acute pancreatitis.
For decades, resolving blockages in the bile duct or pancreatic duct required highly invasive open surgery, requiring long hospital stays and prolonged recovery periods. Today, modern medicine offers a highly effective, minimally invasive alternative: ERCP (Endoscopic Retrograde Cholangiopancreatography). Performed by a dedicated ERCP specialist in Tumakuru, ERCP combines advanced endoscopy with real-time X-ray imaging to diagnose and immediately treat complex disorders of the bile and pancreatic ducts.
Deconstructing the Terms: What Is ERCP?
To truly understand ERCP, it is helpful to break down the medical jargon:
- • Endoscopic: Refers to the use of an endoscope—a thin, flexible tube equipped with a light and camera—passed through the mouth into the digestive tract.
- • Retrograde: Means "backward direction." During the procedure, contrast dye is injected in a direction opposite to the natural forward flow of digestive juices.
- • Cholangio: Relates to the bile ducts, the network of tubes that carry bile from the liver and gallbladder to the small intestine.
- • Pancreato: Relates to the pancreas and the pancreatic duct system.
- • Graphy: Represents the taking of X-ray pictures or radiographic recordings to visualize the anatomy.
Essentially, ERCP allows a skilled gastroenterologist in Tumakuru to guide a special scope (duodenoscope) directly to the exit point of the bile and pancreatic ducts in the small intestine (the papilla), inject a dye, take X-rays, and perform complex therapeutic maneuvers on the spot.
A Therapeutic Tool, Not Just a Diagnostic Test
One of the most important developments in modern gastroenterology is that ERCP is now primarily a therapeutic procedure. In the past, ERCP was frequently used just to examine the bile and pancreatic ducts. However, because ERCP carries small but definite medical risks, non-invasive imaging technologies have now taken over the diagnostic role.
Today, if a doctor only wants to examine the bile ducts, they will recommend a non-invasive scan such as an MRCP (Magnetic Resonance Cholangiopancreatography) or an Endoscopic Ultrasound (EUS). ERCP is reserved for when active intervention—such as removing a stone, clearing an infection, dilating a narrowed duct, or placing a stent—is required. It is a form of highly targeted, precise therapeutic endoscopy.
When is ERCP Needed? Key Indications
An ERCP is indicated when there is a suspected block, narrowing, or leak in the biliary or pancreatic duct systems. The most common conditions requiring ERCP include:
1. Common Bile Duct (CBD) Stones
Gallstones are formed in the gallbladder, but they can slip out into the common bile duct. Once lodged there, they block the flow of bile, causing severe pain, jaundice, and dangerous infections. ERCP is the gold standard for **CBD stone removal**, allowing the specialist to retrieve and pull these stones out into the intestine.
2. Biliary Strictures (Narrowing of the Bile Ducts)
Strictures are abnormal narrowings of the bile ducts. They can be benign (caused by inflammation, surgical scarring, or chronic pancreatitis) or malignant (caused by cholangiocarcinoma, pancreatic cancer, or metastatic tumors). ERCP enables the placement of plastic or metal stents to hold the narrowed duct open and restore bile drainage.
3. Acute Cholangitis (Bile Duct Infection)
When a bile duct is blocked, bacteria can multiply quickly in the stagnant bile, causing a severe, life-threatening infection called cholangitis. Immediate ERCP is critical to drain the infected bile, reduce pressure in the biliary tree, and save the patient's life.
4. Pancreatic Duct Stones and Obstructions
In patients with chronic pancreatitis, stones can form inside the pancreatic duct, blocking the outflow of pancreatic enzymes and causing debilitating chronic pain. During an **advanced endoscopy in Tumakuru**, a specialist can use ERCP to extract pancreatic stones or place stents to bypass strictures.
5. Post-Surgical Bile Leaks
Accidental injury to the bile ducts during gallbladder removal surgery (cholecystectomy) can lead to bile leaking into the abdomen. ERCP can resolve this by placing a temporary plastic stent across the leak site, redirecting the bile flow and allowing the duct to heal naturally.
Symptoms That May Warrant Biliary Intervention
Disorders affecting the **pancreatic and biliary disorders** produce distinct signs. Consult an **endoscopy specialist in Tumakuru** if you experience any of the following symptoms:
The ERCP Procedure: What to Expect
Understanding the stages of the ERCP procedure helps alleviate anxiety. Here is the typical clinical timeline for a patient:
1. Pre-Procedure Preparation
Patients must fast (no food or water) for 6 to 8 hours before the test to ensure an empty stomach. Routine blood tests (coagulation profile, kidney functions) are checked, and instructions regarding blood-thinning medications are provided.
2. Sedation and Positioning
The procedure is performed in an advanced endoscopy suite equipped with a fluoroscopy X-ray machine. The patient lies on their left side or stomach. An anesthesiologist administers conscious sedation or general anesthesia to ensure complete comfort and safety.
3. Scope Insertion and Papilla Location
Dr. Balakrishna carefully passes the duodenoscope down the mouth, through the esophagus and stomach, and into the duodenum (the first part of the small intestine). The scope is positioned directly in front of the Ampulla of Vater, where the bile and pancreatic ducts empty.
4. Cannulation and Contrast Injection
A micro-catheter (cannula) is inserted through the scope and threaded into the bile or pancreatic duct. A contrast dye is injected, and X-ray images are captured immediately. This reveals the exact location of stones, narrowings, or blockages.
5. Therapeutic Intervention (Sphincterotomy & Stone Extraction)
To extract stones, a tiny cut is made in the muscle surrounding the duct opening (sphincterotomy) using a specialized electrosurgical wire. Baskets or balloon catheters are then inserted to sweep the CBD stones out into the intestine. If narrowing is found, a plastic or self-expanding metal stent is placed.
6. Post-Procedure Recovery
The patient is moved to the recovery area and monitored closely for a few hours. Some patients can go home the same day, while others (especially those with complex interventions or active infections) are observed overnight in the hospital.
Understanding CBD Stone Removal
**Bile duct stone treatment** is one of the most common reasons patients are referred for ERCP. When a gallstone moves out of the gallbladder and becomes stuck in the Common Bile Duct (CBD), it acts like a plug in a drain, causing bile to back up.
During the **CBD stone removal** procedure:
- Sphincterotomy: The opening of the duct is safely widened using electrosurgical current to allow passage.
- Balloon Extraction: An uninflated balloon catheter is guided past the stone, inflated, and pulled back, dragging the stones into the intestine.
- Dormia Basket Extraction: For larger or stubborn stones, a wire mesh basket is used to grasp and pull the stone out.
- Mechanical Lithotripsy: If a stone is too large to fit through the opening, a mechanical crusher can break it into smaller fragments inside the duct before removal.
Is ERCP Safe? Risks and Complications
ERCP is an extremely effective therapeutic procedure, but like all advanced medical interventions, it carries a small risk of complications. Being aware of these helps you prepare and make informed decisions:
- • Post-ERCP Pancreatitis (3% to 5% risk): The most common risk. Irritation or temporary swelling near the pancreatic duct can trigger pancreas inflammation. Most cases are mild and resolve with a few days of bowel rest and IV fluids in the hospital. Specialist techniques and medications are used during the procedure to minimize this risk.
- • Bleeding (1% to 2% risk): Can occur after a sphincterotomy (cutting the duct opening). It is usually minor and controlled immediately during the procedure using thermal therapy or clips.
- • Infection (Cholangitis): Can occur if a blocked duct is not fully drained. Administering preventative IV antibiotics before and after the procedure greatly reduces this risk.
- • Perforation (less than 1% risk): A rare but serious complication where a tear is created in the wall of the digestive tract or bile duct. It may require surgical repair or clip placement.
While these risks sound concerning, choosing an experienced **advanced endoscopy specialist in Tumakuru** reduces the likelihood of complications significantly. The procedure is performed with state-of-the-art instruments under strict clinical protocols.
ERCP vs. MRCP: Understanding the Differences
Patients often get confused between ERCP and MRCP because their names are highly similar. However, they serve completely different purposes:
| Feature | MRCP | ERCP |
|---|---|---|
| Nature | Non-invasive MRI Scan | Minimally invasive endoscopic procedure |
| Purpose | Diagnostic only (viewing structures) | Therapeutic (treating blockages/stones) |
| Anesthesia | None required | Conscious Sedation or General Anesthesia |
| Complications Risk | Virtually zero | Low but present (pancreatitis, bleeding) |
| Interventions | Cannot remove stones or place stents | Can extract stones, place stents, take biopsies |
What is Recovery Like After ERCP?
Most patients recover quickly after an ERCP procedure, but following professional medical guidelines is essential to prevent complications:
- Dietary Resumption: You will remain fasting until the sedation fully wears off and your throat reflex returns. Once cleared, you can start with sips of water, progressing to a soft, light diet that is low in fat for the first 24-48 hours.
- Rest: Avoid strenuous physical activity, heavy lifting, or intense exercise for at least 3 to 5 days, particularly if a sphincterotomy was performed.
- Symptom Monitoring: Mild throat soreness, bloating, or gas is normal. However, you should report severe abdominal pain, persistent nausea, high fever, or dark blood in your stool to your doctor immediately.
Frequently Asked Questions
No, ERCP is not an open surgery. It is a minimally invasive, advanced endoscopic procedure. The doctor accesses the bile and pancreatic ducts through the mouth using a flexible scope, meaning there are no external incisions, cuts, or scars on your abdomen.
ERCP is usually performed under deep conscious sedation or general anesthesia. This ensures that you do not feel any discomfort, gagging, or pain during the procedure and remain completely still, allowing the specialist to work safely and precisely.
A typical therapeutic ERCP procedure takes between 30 to 60 minutes, depending on the complexity of the condition, such as the size and number of stones to be removed, or whether a stent needs to be placed.
While some straightforward ERCP procedures can be done on an outpatient basis (allowing you to go home after 4-6 hours of recovery), many patients are kept for overnight observation. This is a safety measure to ensure no complications (like pancreatitis) develop and that you can comfortably tolerate oral fluids.
ERCP can remove stones that are lodged in the common bile duct (CBD). However, ERCP cannot remove stones that are inside the gallbladder itself. Gallbladder stones are treated through a surgical procedure to remove the gallbladder, known as cholecystectomy.
For expert biliary care and ERCP procedures in Tumakuru, Dr. Balakrishna A. is a highly trusted name. Practicing as a Consultant Gastroenterologist and Hepatologist at Siddaganga Hospital, he is highly specialized in advanced therapeutic endoscopy and pancreatico-biliary interventions.
Expert Biliary & Pancreatic Care in Tumakuru
Biliary and pancreatic obstructions require quick medical attention to prevent severe complications like jaundice, sepsis, or pancreatitis. ERCP is a highly effective, safe, and minimally invasive solution that avoids major surgery.
Dr. Balakrishna A. provides cutting-edge advanced therapeutic endoscopy services, including ERCP and stone extractions, in a modern clinical setup with round-the-clock emergency support at Siddaganga Hospital, Tumakuru.